
Silicosis
Silicosis affects more workers than any other respiratory disease. Silicosis has escaped national attention despite its prevalence. Harmful concentrations of dust are invisible and symptoms of silicosis are generic. According to the World Health Organization, under diagnosis and under reporting are frequent. Thousands of American workers suffer unknowingly from the disease.
Silicosis is 100% preventable. The methods of preventing silicosis are simple and have been known for centuries. While European countries banned silica in sandblasting over 50 years ago, American companies continued to make, sell and use silica sand blasting materials. Liable defendants include silica suppliers, premises owners, equipment manufacturers and respirator manufacturers.
Diagnosis of Silicosis
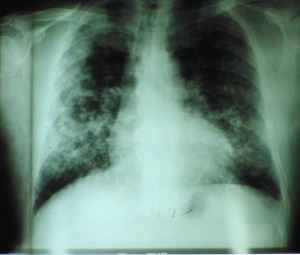
Silicosis is an insidious, progressive lung disease. High exposures can produce acute silicosis with dramatic impairment, and even death, without concomitant fibrosis. At lower exposures, silicosis produces distinct lung scarring, generally rounded opacities and nodules in the upper lobes, as opposed to lower lobe, linear scarring in asbestosis.
Fungal and bacterial infections often complicate silicosis tuberculosis is often a complication with fatal results. Physicians unfamiliar with the disease or a patient’s work history may misdiagnose pulmonary edema or pneumonia rather than silicosis.
History of Silicosis
Ancient Greeks were familiar with lung disease in quarry workers (Hippocrates) and the fact that respirators could prevent the disease (Pliny). Agricola(1566) described disease in stone cutters as later did Ramazini (1713). By 1917, the U.S. Public Health Service identified sand blasters and foundry workers to be at high risk of silicosis. As the 20th century progressed, silicosis was the reference to which newer diseases were compared. See e.g., Lanza, Silicosis and Asbestosis(1935). The Gauley Bridge disaster with 475 deaths in 1931 focused public attention on silicosis in America. Lawsuits in the 1920’s and 1930’s resulted in workers’ compensation coverage for occupational disease.
Trades affected by Silicosis
Silica dust is released during operations in which rocks, sand, concrete and some ores are crushed or broken. Work in mines, quarries, foundries, and construction sites, in the manufacture of glass, ceramics, and abrasive powders, and in masonry workshops is particularly risky.
Sandblasting is one of the high-risk operations for silicosis. Any abrasive blasting, even if the abrasive does not contain silica, may pose a silicosis hazard when it is used to remove materials that contain silica, such as remains of sand moulds from metal castings.
There are three kinds of silicosis, based on amount of exposure and length of time.
Chronic
occurs after 10 or more years of mild overexposure to silica
the most common of all types
may go undetected for years
Accelerated
develops between 5 and 10 years of moderate overexposure
Acute
develops within weeks up to five years due to breathing very large amounts of silica